


Content Warning: This blog article contains references to violence, sexual abuse, and traumatic events. Please be aware that UMGC offers emergency student resources for any student who might require them. We also offer health and wellness resources specifically for veterans.
June is Post-Traumatic Stress Disorder Awareness Month, and June 27 is specifically designated as National Post-Traumatic Stress Disorder Awareness Day. Throughout the month of June, practitioners, educators, government agencies, nonprofit organizations, and individuals across the United States have been thoughtfully advocating for those whose lives have been touched by this treatable disorder.
The following blog is written in the spirit of spreading knowledge and amplifying awareness of post-traumatic stress disorder.
Is post-traumatic stress disorder (PTSD) a condition related only to wartime trauma?
Post-traumatic stress disorder (PTSD) is a clinically diagnosed mental health condition that can occur following a direct experience with—or the witnessing of—a significantly traumatic event. While many people associate PTSD with veterans and wartime trauma, PTSD can develop in response to serious accidents, life-threatening illnesses, natural disasters, mass violent events, physical abuse, and sexual assault during childhood or adulthood.
What is the prevalence of PTSD in the United States?
Approximately 60 percent of men and 50 percent of women in the United States will experience at least one traumatic event during their life1. Within this group, the percentage of those who go on to develop PTSD symptoms is relatively small: about 4 percent of men and 8 percent of women2. These statistics tell us two things. First, that lots of people recover from traumatic experiences3. Second, the prevalence of PTSD in the United States translates to an estimated 12 million adults who have PTSD in any given year4. This is significant.
If the stress symptoms following a traumatic event are common, what makes PTSD unique?
“What makes PTSD unique is that it is seen, in the research, as a ‘failure to recover’ rather than the development of an abnormal response,” said Jacqueline Mahoney, PhD, adjunct assistant professor of psychology at UMGC. “PTSD symptoms immediately after a trauma are normal.”
Examples of these symptoms can include feelings of stress, anger, and fear. The intensity and duration of the symptoms vary and can make anyone feel momentarily off-balance or jittery.
Those who are poised for recovery will begin to feel better within a few weeks or months immediately following the trauma5. Those who are gravitating towards a diagnosis of PTSD, however, might begin to wonder when they will experience recovery. Periodic or daily triggers such as loud sounds, smells, people, environmental cues, or intrusive thoughts might persist. These triggers can agitate the stress response to a person’s trauma.
Anonymous, sharing how environmental cues and intrusive thoughts months following a life altering trauma have impacted someone close to them.

It is important to note that the signs of PTSD may appear at any time. For some, symptoms may appear soon after the trauma and continue until help is sought. Others may not develop symptoms until months or even years after the traumatic event6.
How are individuals diagnosed with PTSD?
To be diagnosed with PTSD, an individual must express symptoms for more than one month from the following four distinctive7 subgroups:
- Re-experiencing symptoms, which entails unwelcome, distressing trauma event memories, nightmares, flashbacks and strong reactions to trauma reminders.
- Avoidance symptoms, which include intentional avoidance of trauma memories, thoughts or reminders.
- Negative alterations of cognitions and mood, which address memory lapses, persistent negative expectations of the world, and disruption of feelings of trust and connection with self and others.
- Hyperarousal symptoms, which are expressed though anger, irritability, recklessness, hyper alternes and disruptions in sleep or concentration.
Dee Preston-Dillon, PhD, an adjunct professor of psychology at UMGC, shared the following account of the expression of PTSD symptoms:
My initial understanding came in the mid-1970s, while teaching psychology to undergraduate students on military bases in Hawaii, families with direct experience from the Vietnam War. Their stories were pressed with deep grief, rage, images of death, deep loss, anxiety, crisis with acceptance in the culture at large, and survivor’s guilt. Over the decades, these stories changed very little. Existential suffering continued. Depression, uncontrolled terrifying images, social and cultural displacement, child and spouse abuse, and suicide are only part of the experience for PTSD and complex PTSD8.
Do different groups experience higher rates of PTSD?
Research dedicated to PTSD concludes that the development of PTSD symptoms is prevalent in multiple trauma-exposed populations. These populations can include:
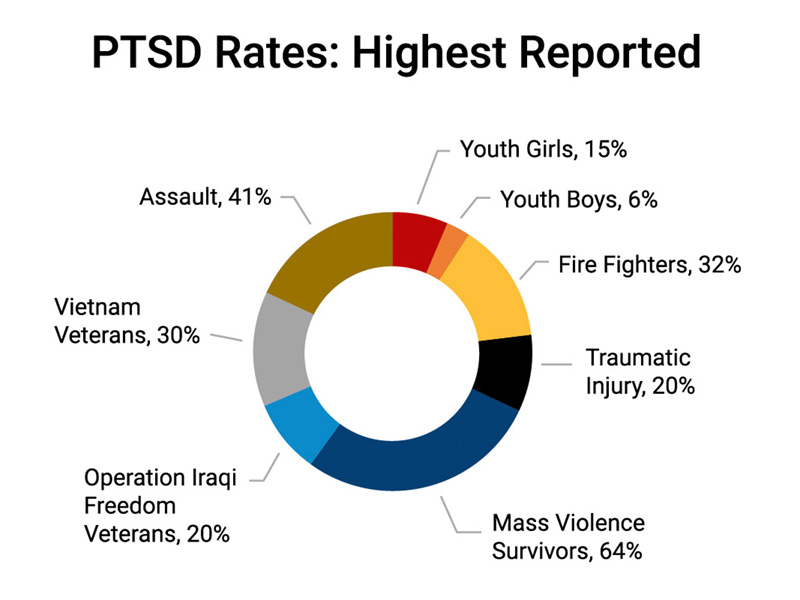
Youth. According to the National Center for PTSD9, approximately 15 to 43 percent of girls experience at least one trauma. The number for boys is remarkably similar: 14 to 43 percent of boys will experience at least one trauma. Of those youth who have had a trauma, 3 to 15 percent of girls and 1 to 6 percent of boys develop PTSD. It should be noted that a child’s risk of developing PTSD may be influenced by the severity of the trauma, proximity to the traumatic event, and the parents’ reactions to the trauma.
Sexual Assault Victims. A recent literature review found that PTSD is common and severe following sexual assault10. Across a sample of 2,106 cases, 74.58 percent of the individuals met the diagnostic criteria for PTSD one month following trauma, and 41.49 percent did 12 months following sexual assault. Within this sample, it was found that most symptom recovery occurred within the first three months following trauma, after which the rate of recovery slowed.
Mass Violence Survivors. Mass violent events can lead to a wide range of expressed reactions by direct victims, emergency personnel, and the community at large. Empirical evidence suggests that up to 95 percent of mass-shooting survivors experience PTSD symptoms at any level11. In the months that follow, the demonstrated prevalence of PTSD among mass violent trauma survivors ranges from 11.7 percent to 64 percent12.
Firefighters. Research co-authored by Brooke Bartlett, PhD, adjunct assistant professor of psychology at UMGC, notes that U.S. firefighters have an estimated lifetime PTSD prevalence rate of 32.4 percent13. This is three times higher than the prevalence rate of 8.3 percent within the general population14.
Traumatic Injury/Illness Victims. Each year, traumatic injuries affect 2.6 million adults in the U.S., which contributes to extenuating health challenges. According to the American College of Surgeons, these injuries put trauma patients at risk for PTSD at rates as high as 20 to 40 percent15. For individuals who survive an acute life-threatening medical event (e.g., cancer) it is thought PTSD occurs in 12 to 25 percent. Newly released research by Vanessa Young, adjunct instructor with the psychology program at UMGC, and colleagues, suggests that there may be underappreciated differences between PTSD linked to medical trauma versus psychological trauma16. The differences may be due to acute injury or disease manifestations that are enduring and contribute to the maintenance of PTSD symptoms17.
Veterans. According to the National Center for PTSD,18 PTSD prevalence among recent war veterans can vary. Between 11 and 20 percent of Operation Iraqi Freedom and Operation Enduring Freedom veterans may express PTSD symptoms during their lifetime. PTSD prevalence projections for Gulf War (Desert Storm) veterans is 12 percent in a given year, and 30 percent for Vietnam veterans within their lifetime.
The good news: PTSD is treatable!
For anyone currently living with PTSD, there is good news: “PTSD is treatable!19” said Jacqueline Mahoney, PhD, adjunct assistant professor of psychology at UMGC. For many individuals, PTSD treatment can alleviate symptoms. For others, the intensity or occurrence of their symptoms may be reduced.
Evidence-based psychotherapies for treating PTSD include first-line treatments such as:
- Cognitive Processing Therapy (CPT). CPT is a 12-session psychotherapy for PTSD. CPT teaches clients how to evaluate and change upsetting thoughts held since the targeted trauma. By changing thoughts, one can change how they feel.
- Prolonged Exposure (PE). PE teaches clients to gradually approach trauma-related memories, feelings and situations that have been avoided since the trauma event.
- Eye Movement Desensitization and Reprocessing (EMDR). EMDR helps a client process and make sense of their trauma while also paying attention to a back-and-forth movement or sound (like a finger waving side to side or a tone). The “focusing task” shifts the way that the client experiences trauma-related memories.
- Cognitive Behavior Therapy (CBT). CBTs that are specific for PTSD can help the client learn how to change unhelpful behaviors or thoughts.
These therapies and others (e.g., select medicinal therapies) are demonstrated to aid in PTSD recovery20.
Opportunities to improve PTSD outcomes can drive research and therapeutic best practices.
To improve the efficacy of PTSD treatment options, researchers and practitioners are applying innovative solutions. Positive efforts include condensing treatment sessions into fewer weeks (known as intensive interventions) and expanding therapies to address emotion regulation (which appears to support both psychological and physiological responses to stress).21 Also, interactive therapies like Equine Assisted Therapy22 and expressive therapies (e.g., Sand Therapy) are creating safe, constructive therapeutic spaces that facilitate expression beyond talk therapies23.
As we begin to understand more about PTSD, expanding therapeutic options will increase participant completion rates among those most likely to drop out of therapy (e.g., individuals younger than 30-35 years of age, participants balancing life challenges)24. New options will also improve recovery outcomes, due to greater sensitivity to the unique impact that different types of traumas (manmade, medical, natural disaster, discrete, reoccurring) produce.
PTSD today and into the future
PTSD is still impacting lives and the fabric of communities. This year, millions across the United States will experience a life-altering trauma and PTSD symptoms. Most will recover within a few weeks. Others will find recovery through the support of family, friends, their community, and a trained specialist knowledgeable in PTSD therapies.
Awareness of the disorder is more important today than ever. Awareness helps individuals recognize the symptoms and to open dialogues in support of healing. It also highlights that there is a critical national need for a specialized workforce, dedicated to leveraging the principles of psychology, the social sciences, and nursing in order to deliver much needed mental health interventions.
Employment of behavioral disorder and mental health counselors is projected to grow 23 percent from 2020 to 203025. Vanessa Young, adjunct instructor with the psychology program at UMGC, has noted that the number of PTSD diagnosis may continue to grow26. This is partly due to the number of individuals who have experienced mild to severe COVID-19 symptoms or will experience delayed symptoms27.
Therapies do offer promise for PTSD recovery. New research and applied interventions are being explored. The future of the disorder, understanding it and treating it, requires training tomorrow’s thought leaders and therapists today.
UMGC offers career-relevant degrees in fields that deal with these topics, including psychology and healthcare & science. Students looking to embrace this call for action and for understanding will find flexibility, workplace-relevant education, and expanded credentialling opportunities at UMGC.
1 “How Common Is PTSD in Adults?” National Center for PTSD. Retrieved June 3, 2022, from https://www.ptsd.va.gov/understand/common/common_adults.asp
2 “How Common Is PTSD in Adults?” National Center for PTSD. Retrieved June 3, 2022, from https://www.ptsd.va.gov/understand/common/common_adults.asp
and
Lehavot, K., Katon, J. G., Chen, J. A., Fortney, J. C., & Simpson, T. L. (2018). “Post-traumatic stress disorder by gender and veteran status.” American Journal of Preventive Medicine, 54(1), e1–e9. https://doi-org.ezproxy.umgc.edu/10.1016/j.amepre.2017.09.008
3 Mahoney, J. (2022, May 23). Personal communication.
4 “How Common Is PTSD in Adults?” National Center for PTSD. Retrieved June 3, 2022, from https://www.ptsd.va.gov/understand/common/common_adults.asp
5 “Understanding PTSD and PTSD Treatment.” National Center for PTSD. U.S. Department of Veteran Affairs. Retrieved June 15, 2022, from https://www.ptsd.va.gov/publications/print/understandingptsd_booklet.pdf
6 “What To Look For: Post-Traumatic Stress Disorder.” Retrieved June 3, 2022, from https://www.samhsa.gov/mental-health/what-is-mental-health/conditions/ptsd
7 “What is Posttraumatic Stress Disorder (PTSD)?” APA. Retrieved June 3, 2022, from https://psychiatry.org/patients-families/ptsd/what-is-ptsd
8 Preston-Dillon, D. (2022, May 23). Personal communication. Complex PTSD involves multiple, potentially extended trauma events. In 2018, the World Health Organization (WHO) published diagnostic criteria for complex PTSD in its International Statistical Classification of Diseases and Related Health Problems (11th Revision).
9 “How Common is PTSD in Children and Teens?” National Center for PTSD. Retrieved June 13, 2022, from https://www.ptsd.va.gov/understand/common/common_children_teens.asp
10 Dworkin, E. R., Jaffe, A. E., Bedard-Gilligan, M., Fitzpatrick, S. (2021). “PTSD in the year following sexual assault: A meta-analysis of prospective studies.” Trauma Violence Abuse. Epub ahead of print. doi: 10.1177/15248380211032213.
11 Littleton, H., Kumpula, M., & Orcutt, H. (2011). “Posttraumatic symptoms following a campus shooting: The role of psychosocial resource loss.” Violence and Victims, 26, 461–476. http://dx.doi.org/10.1891/0886-6708.26.4.461
12 Hafstad, G. S., Dyb, G., Jensen, T. K., Steinberg, A. M., & Pynoos, R. S. (2014). ”PTSD prevalence and symptom structure of DSM–5 criteria in adolescents and young adults surviving the 2011 shooting in Norway.” Journal of Affective Disorders, 169, 40–46. http://dx.doi.org/10.1016/j.jad.2014.06.055
13 Tomaka, J., Magoc, D., Morales-Monks, S. M., & Reyes, A. C. (2017). ”Posttraumatic stress symptoms and alcohol related outcomes among municipal firefighters.” Journal of Traumatic Stress, 30(4), 416–424. https://doi.org/10.1002/jts.22203
14 Kilpatrick, D. G., Resnick, H. S., Milanak, M. E., Miller, M. W., Keyes, K. M., & Friedman, M. J. (2013). ”National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria.” Journal of Traumatic Stress, 26(5), 537–547. https://doi.org/10.1002/jts.21848
15 “Statement on Post-Traumatic Stress Disorder in Adults.” American College of Surgeons. Retrieved on June 13, 2022, from https://www.facs.org/about-acs/statements/ptsd-in-adults/
16 Gimigliano F, Young VM, Arienti C, Bargeri S, Castellini G, Gianola S, Lazzarini SG, Moretti A, Heinemann AW, Negrini S. (2022, June 19). “The Effectiveness of Behavioral Interventions in Adults with Post-Traumatic Stress Disorder during Clinical Rehabilitation: A Rapid Review.” International Journal of Environmental Research and Public Health, 19(12):7514. https://doi.org/10.3390/ijerph19127514
17 Edmondson D. (2014). “An enduring somatic threat model of posttraumatic stress disorder due to acute life-threatening medical events.” Social and Personal Psychology Compass, 5, 118-134. doi: 10.1111/spc3.12089. PMID: 24920956; PMCID: PMC4048720. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4048720/
18 “How Common is PTSD in Veterans?” National Center for PTSD. Retrieved June 3, 2022, from https://www.ptsd.va.gov/understand/common/common_veterans.asp
19 Preston-Dillon, D. (2022, May 23). Personal communication.
20 “Management of Posttraumatic Stress Disorder, Work Group.” (2017). VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder (version 3.0 ed.). Department of Veterans Affairs and Department of Defense. Retrieved from https://www.proquest.com/reports/va-dod-clinical-practice-guideline-management/docview/1916311898/se-2?accountid=28179
and
Steenkamp, M. M., Litz, B. T., & Marmar, C. R. (2020). “First-line psychotherapies for military-related PTSD.” Journal of American Medical Association, 323, 656. Advanced online publication. https://doi.org/10.1001/jama.2019.20825
21 Mathersul, D. C., Dixit, K., Schulz-Heik, R. J., Avery, T. J., Zeitzer, J. M., & Bayley, P. J. (2022). “Emotion dysregulation and heart rate variability improve in US veterans undergoing treatment for posttraumatic stress disorder: Secondary exploratory analyses from a randomized controlled trial.” BMC Psychiatry, 22(1), 1–12. https://doi-org.ezproxy.umgc.edu/10.1186/s12888-022-03886-3
22 Fisher, P. W., Lazarov, A., Lowell, A., Arnon, S., Turner, J. B., Bergman, M. & Neria, Y. (2021). “Equine-assisted therapy for posttraumatic stress disorder among military veterans: An open trial.” The Journal of Clinical Psychiatry, 82(5), 36449. https://www.psychiatrist.com/news/exploring-equine-assisted-therapy-for-ptsd-in-military-veterans/
23 Preston-Dillon, D. (2022, May 23). Personal communication.
24 Sciarrino, N. A., Bartlett, B. A., Smith, L. J., Martin, C. E., & Williams, W. (2022). “Factors contributing to PTSD treatment dropout in veterans returning from the wars in Iraq and Afghanistan: A systematic review.” Psychological Services, 19(1), 183–200. https://psycnet.apa.org/record/2021-22806-001
25 U.S. Bureau of Labor Statistics. Accountants and auditors. (2022). Occupational Outlook Handbook. Retrieved June 3, 2022, from https://www.bls.gov/ooh/community-and-social-service/substance-abuse-behavioral-disorder-and-mental-health-counselors.htm
26 Young, V. (2022, May 23). Personal communication.
27 Young, V. (2022, May 23). Personal communication.
Reference on this webpage to any third-party entity or product does not constitute or imply endorsement by UMGC nor does it constitute or imply endorsement of UMGC by the third party.